
Inverted nipples are often a normal anatomical variation present from birth, but a newly inverted nipple should always be medically evaluated. This guide explains the common causes, grades, and symptoms of nipple inversion. It also covers non-surgical and surgical treatment options, including breastfeeding considerations. Learn the warning signs that require prompt medical attention to protect your breast health.
A nipple is made up of milk ducts, smooth muscle, nerve endings, and connective tissue. Normally, the nipple projects outward. In some people, the milk ducts are slightly shorter than usual, or fibrous tissue beneath the areola (the dark skin around the nipple) pulls the nipple tip inward, giving it a dimpled or tucked-in appearance.
So, if you have noticed that one or both of your nipples point inward rather than outward, you may have inverted nipples. It is a normal anatomical variation that is present since birth in some people.
Inverted nipples can also change in how they look throughout the day due to temperature, touch, or hormonal shifts. This is completely normal.
| Congenital Inversion | Acquired Inversion |
|
|
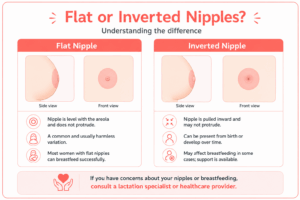
No. A flat nipple lays evenly with the surrounding areola. It does not project outward, but it does not retract inward either. An inverted nipple is actively pulled inward.
The two can look similar but have different implications for breastfeeding and treatment.
First, understand what has caused your nipple inversion. Some most common causes of such nipple type are:
These two conditions can also cause scarring that retracts the nipple inward.
If you have had breast surgery, a biopsy, breast reduction, or radiation therapy in the past, scar tissue from those procedures can sometimes affect the surrounding ductal tissue and cause the nipple to retract. This type of inversion is usually stable over time.
As we get older, breast tissue naturally loses some of its elasticity. This can lead to mild nipple retraction in older women. It is gradual, affecting both sides, and not linked to any underlying condition. It is a natural part of how breast tissue changes with age.
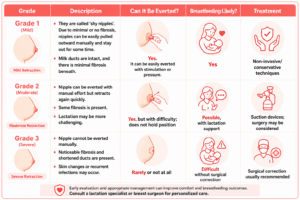
It is divided into three grades based on the degree of fibrosis.
Grade 1 (Mild)
Grade 1 inverted nipples are sometimes called ‘shy nipples.’ They can be easily pulled outward with light pressure or stimulation and stay out for a little while on their own. The milk ducts are fully intact with little to no fibrous tissue. Breastfeeding is very much possible at this grade.
Grade 2 (Moderate)
At Grade 2, the nipple can still be everted with some manual effort. However, it retracts back quickly. There is some fibrosis present beneath the nipple. Breastfeeding is possible but may need extra support.
Grade 3 (Severe)
Here, the nipple cannot be everted manually at all. There is noticeable fibrosis and shortening of the milk ducts beneath. Surgery is generally the recommended path forward at this stage.
Most people with congenital inverted nipples (those who have since birth) have Grade 1 or Grade 2 inversion. Grade 3 is less common and is more frequently associated with acquired causes such as chronic infection or significant fibrosis.
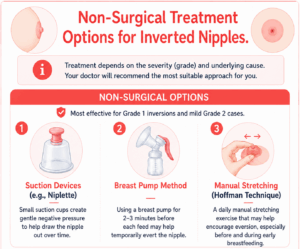
The treatment for inverted nipples depends majorly on its grade and the root cause. Based on your overall condition, you may be suggested any of these treatment approaches.
Most effective for Grade 1 inversions and mild Grade 2 cases.
There are two approaches your breast surgeon may discuss with you:
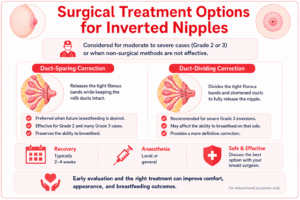
Important: If you are considering nipple correction surgery and have any future plans to breastfeed, discuss this before the procedure, not after. Your surgeon needs to know, as it affects which technique is used. Once duct-dividing surgery has been performed, breastfeeding on that side is generally no longer possible.
You should see a doctor promptly if you notice:
If you have had lifelong inverted nipples, no new symptoms, and no other breast changes, a routine mention to your doctor is sufficient. The breast care specialist will advise on regular breast screening as appropriate for your age and risk profile.
If you have noticed a recent change in your nipple and are struggling to figure out the reason behind it, the expert team of experienced breast specialists, gynecologists, and reconstructive surgeons at the CK Birla Hospital is here to help you. Our dedicated ‘Breast Centre’ provides compassionate care in a safe and private setting. You can book a consultation for early detection.
Is an inverted nipple normal?
Yes. When it has been present since birth or adolescence and has not changed, a bilateral inverted nipple is a normal anatomical variation. But if your nipple has recently changed, that is when a medical evaluation is needed.
Can a nipple become inverted after pregnancy or breastfeeding?
Yes, this can happen. Breastfeeding puts the breast through significant changes such as engorgement, repeated feeding, and eventual deflation of breast tissue. All of these changes can occasionally alter the way the nipples are present. Repeated breast infections (mastitis) during breastfeeding can also leave behind minor scarring that gradually draws the nipple inward.
Can you breastfeed with inverted nipples?
Women with Grade 1 inversion can usually breastfeed without any intervention. Those with Grade 2 inversion may succeed with practical support such as using a breast pump before feeds to temporarily evert the nipple, or wearing nipple shields during feeding. Grade 3 inversion makes breastfeeding more challenging, and surgical correction may be discussed with this goal in mind.
What age do nipples usually invert?
Congenital nipple inversion is first noticed during puberty, when breast development begins and the nipple architecture becomes apparent. Some people notice it only in adulthood. If nipple inversion appears for the first time in a woman over 40 with no prior history, this should always be evaluated without any delay.
Written and Verified by:

Similar The Breast Centre Blogs
Request a call back




