A 47-year-old international patient came to Dr Mayank Madan for a consultation with the following problems:
Based on the patient’s age and condition, further investigative procedures were carried out to get a clear picture of the problem.

An Upper GI Endoscopy was performed which revealed Hiatal Hernia with a dilated stomach and mesentero-axial volvulus. Simply put, there was an abnormal rotation of more than 180 degrees, around a transverse axis connecting the middle of the greater and lesser curvatures of the stomach. This was due to the protrusion of the stomach, through the oesophagal opening in the diaphragm.
Further, a Barium meal study was performed which revealed mild luminal attenuation with mucosal irregularity in the middle of the stomach. There was no existence of any significant obstruction most likely as a result of previous GIST surgery. Based on these findings the patient was diagnosed with Hiatal Hernia with gastric volvulus.
Upon careful assessment of the findings, Dr Mayank Madan and his team decided on performing the Laparoscopic Hiatal Repair with Dor’s Fundoplication and Gastropexy done under general anaesthesia.
During surgery, it was found that there were dense omental and bowel adhesions due to the existence of a previous midline scar. To avoid causing any bowel injury, an adhesiolysis was performed to meticulously avoid any complications due to injury.
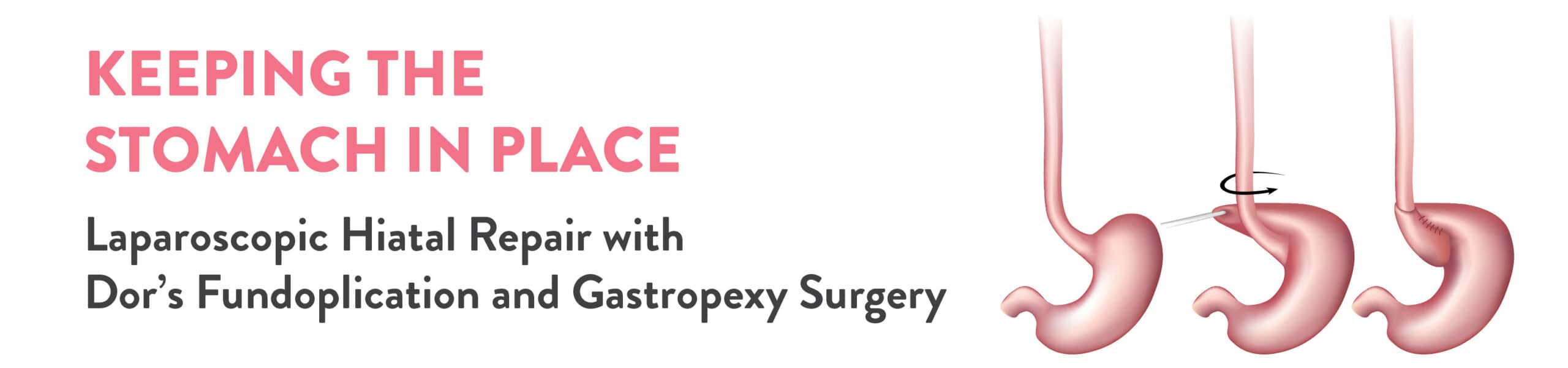
Further, the whole of the greater curvature of the stomach was stuck to the left lobe of the liver, causing the volvulus. To repair this, a meticulous dissection of adhesiolysis was performed to separate the organs, which led to the derotation of the volvulus formed. There was approximately 3 cm of hiatal defect noted. This was repaired by pulling back the derotated stomach into the abdominal cavity during gastropexy.
During the gastropexy, an anterior wrap of 180 degrees was made and a bougie (36F) was manoeuvred into the stomach cavity. It was suspected that the middle of the stomach might be narrowed due to the hernia, but the bougie could be successfully cleared past the suspected area. Finally, three transfascial sutures were made to secure the stomach to the abdominal wall or the diaphragm. This will further prevent the stomach from moving up into the chest cavity.
The long and eventful surgery was executed successfully without any further injury or operative complications thanks to the laparoscopic approach. Post-surgery, the patient was managed with IV fluids, IV antibiotics, IV antacids, analgesics and other supportive measures to ensure the digestive system is back on track.
Diet was a vital part of the post-operative care, which was mostly liquid from the next day of the surgery. The patient responded well to the surgery and no further complications surfaced. Within 48 hours of the surgery, the patient was discharged as he was hemodynamically stable and showed good signs of recovery.
During the first follow-up after one week, his port site staples were removed and he was sustaining his liquid diet with no complaints of regurgitation. We are happy to have helped another patient regain their health and attain proper relief from their prolonged discomfort.