Filter :

Understanding your menstrual cycle and selecting the right sanitary product to use goes a long way in deciding how comfortable you would be during your periods.
Every girl and woman may experience menstruation differently. While some girls may experience unpleasant symptoms such as menstrual cramps, mood swings, breast tenderness, heavy flow and long periods, others may hardly notice their periods. In both cases, knowing what is unusual is important in detecting any menstrual disorder.
In this article, Dr Anjali Kumar – leading gynaecologist and obstetrician in Delhi NCR, explains all about menstruation and shares tips on selecting the right sanitary product.
Table of Contents
Menstruation, more commonly known as periods, is the natural process of your body discarding blood and tissue from your uterus through your vagina. It generally occurs every month.
Menstruation or periods occur due to our “menstrual cycle”. Let us understand this in further detail.
Every woman is born with two ovaries, each of which contains several immature eggs or oocytes. During the menstrual cycle, the ovaries also produce hormones: oestrogen and progesterone, in order for the oocytes to mature into ova (matured eggs). Only matured eggs can be fertilised for a pregnancy.
These hormones also help your uterus prepare for a pregnancy every month by making the uterine lining or endometrial lining thick and spongy. In case of pregnancy, the resulting embryo attaches itself to the thick uterine lining and continues to grow. This lining is made of tissue and blood. If pregnancy doesn’t happen, the body proceeds to expel this excess lining through the vagina in the form of your monthly period.
Menstruation generally starts after the age of 12-14 years of age. However, it can begin earlier or later as well. If the start of periods is delayed beyond the age of 16 years, a gynaecological checkup is recommended. In many cases, periods may start around the same age as it did for the mother, sisters or other close female relatives of the child.
For any woman or girl of menstruating age, stocking up sanitary products every month is routine. Selecting the right sanitary product is a significant deciding factor about how comfortable you would be during your periods. These products have evolved greatly over the years. We now have alternatives for every body type, the intensity of flow and personal preferences. The most prevalent sanitary products available in the market today are
Pads or sanitary napkins are probably the oldest and most basic type of sanitary product. The first pads can be traced as far back as the late 1800s with the introduction of the first disposable sanitary pad was called the Southball pad.
Pads are rectangles of absorbent material that is used to catch menstrual blood. Over the years, their design has been developed to reduce staining and rashes during menstruation. They come in different sizes and shapes to suit body type and flow intensity. Variations have also been developed to suit different activities (such as a different pad to use while sleeping at night). You may need to try different brands and types of sanitary napkins or pads to find the ones that suit you the best.
You may also come across pads which are perfumed to mask the smell of menstruation. However, these can cause rashes and irritate the delicate skin of the vagina in some women, hence they should be used with greater caution. Remember to change your pad regularly every 3-4 hours even if you are experiencing light flow. Prolonged use of the same pad increases the risk of infections and rashes on the vaginal area.
How to use Sanitary Pads
Remove the sanitary pad from the outer cover and unfold it.
One side of the sanitary pad is absorbent while the other side has adhesive. Place the pad in your underwear, while keeping the absorbent side facing upwards. Press it firmly to make it stick to your underwear.
Change your pad every 3-4 hours (earlier in case of heavy flow).
Tampons are small cylindrical tubes made out of compressed absorbent material with a thread at one end. Based on their size, they can be suitable for heavy to light flow. You may also have to use different sizes of tampons based on the day of your menstruation.
Tampons are inserted into the vagina to absorb menstrual flow from inside. The thread is left outside the vagina and is used to pull the tampon out after use. Tampons can also come with applicators for ease of use.
How to use Tampons
Remove the tampon from the outer cover.
Wash you hands and gently insert the tampon into the vagina. It might take a few extra tries at first.
Once the tampon in inside the vagina, you should not be able to feel it. If you still experience discomfort, it might be because of incorrect insertion. In this case, pull out the tampon with the help of the thread and try inserting a fresh one.
While some girls prefer to squat while inserting the tampon, you may have to experiment to find the position that is most comfortable to you.
Remember to change the tampon often to prevent Toxic Shock Syndrome (TSS)-a rare but extremely dangerous complication.
Menstrual cups are a fairly recent innovation in the field of sanitary products. Like tampons, they are inserted into the vagina. However, rather than absorbing the menstrual discharge like the tampon, it catches and blocks the flow. Menstrual cups are made of soft, bendable silicone or rubber. They are funnel-shaped with a sealed tail end. Once inserted in the vagina, it unfolds and catches the blood flow. Every couple of hours, it has to be removed, drained, washed and reinserted. One of the main advantages of menstrual cups is that it can be reused. Maintaining hygiene is extremely important in this case.
How to use menstrual cups
Wash the menstrual cup thoroughly.
Pinch the top part of the cup between your thumb, index finger and middle finger to fold it.
Gently insert it into the vagina till the tail end. Once it is comfortably inside, remove your fingers. The cup should unfold inside the vagina. In case it doesn’t, remove it and try again after changing your position. Squatting is recommended.
Using the right sanitary product can make your period much easier or much more difficult. The right fit depends on a number of factors. Your build, your flow, the day of your cycle, what you’re doing etc.
Tampons have to be changed often. Hence, using them at night is not advised. Some girls also prefer to use large, winged pads at night to minimise the risk of staining and have more freedom to move in their sleep.
Many girls also prefer pads as they are less invasive. They are easier to use (however, practice makes it easier to use tampons and cups as well) and change. Tampons and cups are popular due to their small size and greater comfort. While pads may cause rashes as well as become uncomfortable and bulky as they get saturated, you generally dont feel tampons and cups once they are inside the vagina. Pads are also unsuitable for activities such as swimming.
Keep the above factors in mind while choosing which sanitary product to use. Don’t be afraid of experimenting. It may take some tries to get it right but once you do, your periods are going to be much more easier on you. The right sanitary product can also have a slight impact on the severity and length of your menstrual cycle. While the choice depends solely on your comfort at the end, your gynaecologist can help you understand your periods better.
Hygiene is the most important thing to keep in mind while menstruating. During this time, you are more prone to getting infections and UTIs. If care is not taken, these problems can become recurrent and extremely severe.
Regardless of which sanitary product you are using, change or wash it (as applicable) every few hours. Wash your vagina thoroughly with water and soft soap. Dry it and then use the pad, tampon or cup.
Extra care needs to be taken while using tampons and cups, and people may tend to forget them in there. Tampons are also associated with a rare and dangerous complication called toxic shock syndrome. Its symptoms include sudden high fever, low blood pressure, vomiting, diarrhea, rash, confusion, muscle aches, redness in the eyes, mouth and throat as well as seizures. Seek medical attention immediately if you notice any of these symptoms.
It may take some time to understand your menstrual cycle and menstruation. Take your time and observe your flow and dont be scared to experiment. Talk to your gynaecologist for more help in deciding the right product. Tracking your menstrual cycle with the help of mobile apps or the simple calendar, can also help you stock up on time and not be caught unawares.
Most importantly, don’t hesitate to Talk about Menstruation.
Connect with our gynecologist in gurgaon if you have the above mentioned symptoms.

COVID-19 has not spared even a single person from its aftermath. For most of the working population, the aftereffects have come in the shape of ‘remote working’. While working from home has a whole bunch of benefits, it also has a few drawbacks. Neck and back pain tops the list of disadvantages of home-based working. In this article, we have compiled some tips to prevent back pain during work from home.
Here is the best work from home guide from Dr Praveen Tittal, a leading shoulder and sports injury specialist at the CK Birla Hospital.
In the face of worldwide lockdown, corporations have asked their employees to operate from homes. Interestingly enough, people have found creative ways to benefit from this situation.
There is a full package of advantages of teleworking. For instance,
However, staying back at home for several months has transformed us into couch potatoes. You are attracting musculoskeletal problems as you grow more relaxed in the new norm. An increasing number of people are experiencing debilitating pain in their back.
You can easily prevent back pain while working from home by practicing these tips.
Maintaining a healthy back is all about lifestyle changes. You will have to give up on the sedentary way of life that you have been practicing so far.
WFH back pain can be avoided effortlessly with the help of these tips and tricks:
Remote working gives you the liberty to work while sitting, standing or even lying down. However, this home rule can be very costly for your back. Just because you can work from your bed, does not mean that you should.
It is suggested that you set out a distinct work station for office hours. It could be your living room, study room or even balcony. The idea is to get out of bed and work while maintaining a good posture.
You may be surprised to learn but your couch or sofa is not the best place for work. If you wish to hold a good posture that supports your back, then you would require a chair that helps you sit comfortably straight and upright.
You should avoid sitting on soft and fluffy furniture. You should lean forward towards your screen or slouch back in your chair.
One of the ways on how to reduce back pain while working from home is to stretch. You should start your day with basic stretching exercises with additional focus on the back. Stretching your back in the morning will help you begin your day with a good body form.
When sitting upright, your lower spine will feel most stress and pressure. It is, thus, important to provide extra support to the lower back. You can simply roll a towel or use a log-shaped pillow to help maintain the posture and decrease the pain.
This work from home advice is not restricted to WFH. You can also practice it while sitting in your office chair when the lockdown reopens.
You should aim to keep your computer screen on a table that offers a straight view. If the height of your screen is too high or low, you will most likely suffer from neck strain.
This strain can further expand into the back and the shoulder. Your neck should be positioned at a straight level for maintaining healthy back.
One of the cons of work from home is restricted to bodily movements. You only required a system and internet to complete your day-long tasks. However, moving your body is just as important as keeping a good posture.
If you sit consistently for long hours, your body will start to feel stiff. It is advised that you make short movements throughout the day. You can set an alarm for each hour that reminds you to take a walk within the house.
A few exercises can be done to prevent back pain while working from home. These exercises do not require spacious workout areas and are ideal for indoors.
Other exercises that can help you maintain a good form are knee to chest stretches, side planks, leg raises and more.
A wrong idea that wrist support is helpful is doing rounds on the internet. You should not provide soft support to your wrists while working on your computer screen.
Tender assistance to the wrists can add compression to the finger tendons. This compression can escalate into pain and affect your shoulders, neck and back.
Among the topmost tips to prevent back pain during work from home is to keep your feet on the floor. You should avoid dangling your feet in the air.
It is also suggested that your feet are not above the screen’s height. The possibility of back pain increases with such postures. You should keep your feet straight on the floor or a footstool.
Some people believe that standing while working will keep them safe from musculoskeletal conditions. However, standing for prolonged hours can cause back problems just like sitting the whole day. The key is to moderate move and maintain the right body position.
You can gradually learn how to maintain a healthy back by following this work from home guide. For more suggestions or tips to prevent back pain during work from home, book an appointment with Dr Praveen Tittal, shoulder and sports injury specialist at the CK Birla Hospital.
Also, read: Tips to keep your back healthy and straight

Each year, with the onset of cold-weather, Indian households prepare to battle winter health hazards. Our mothers gear up with the traditional chyawanprash, monkey caps and vegetable soups to protect us from seasonal health concerns. This winter season, however, we might need to carry out additional protection.
The world is still struggling with COVID-19. We cannot afford to attract winter worries and health hazards during this pandemic. It is because some of the symptoms of these conditions overlap.
If you cough once at your workplace, people will look at you with major suspicion. The greatest concern is that even you wouldn’t know if it is a common cold, flu or coronavirus.
In the article below, Dr Rajiva Gupta, a prominent Internal medicine specialist, addresses the topic of cold-weather health hazards.
Table of Contents
On one hand, the change in season brings reasons to celebrate. With festivities like Diwali, Christmas and New Year arriving during the winters, there are more opportunities to get together for merrymaking. However, on the other hand, these gatherings bring along an increased risk of health issues.
The blow of cold wind can transfer several problems. Common cold-weather health hazards to avoid are:
The set of these conditions is commonly known as winter illnesses. The prevalence of winter illnesses significantly increases if precautionary measures are not taken.
As people spend more time indoors, the likelihood of infection transmission escalates. These numerous viruses can travel through air droplets. Cold weather also leads to more number of acute illnesses. There are certain types of viruses that can affect the throat, mouth or nose.
The signs and symptoms of a common cold are coughing, runny and stuffed nose, congestion in the throat, fatigue, sneezing and fever. Some of these symptoms match the signs of coronavirus. For instance, dry cough, fever and fatigue. This is why you should aim to completely avoid the common cold, flu and catching viruses.
Winter worries and health hazards are not restricted to communicable diseases. During the cold season, a large number of people experience excessive skin dryness. The humidity in the air outdoors drops notably and causes the skin to dry.
The parched and dried up skin can further cause itching. You can see your skin turn red and rough during this season.
One of the most common winter health hazards is the high prevalence of joint pains. This is especially frequent in elder people who suffer from arthritis.
It is because there is a sudden drop in the atmospheric pressure outside. This drop makes the joints more sensitive to pain. People who live with other musculoskeletal disorders may also experience heightened ache and stiffness.
You must have noticed a sudden change in your mood when the weather changes. A large number of people experience seasonal depression or ‘winter blues’. This condition is medically called Seasonal Affective Disorder (SAD).
It is primarily because there is less sun exposure. Studies have shown that our bodies respond differently to daylight when the cold weather begins. As winter days are comparatively short and dark, there is a shift in mood during this time of the year.
Frostbite is a condition when the tissues right under the skin freezes due to a drop in temperature. It is an important cold-weather health hazard to avoid, especially for people who have sensitive skin types.
Frostbites are not very common among the Indian population. However, it affects the more exposed small parts of the body like fingers. The early warning signs of frostbite include numbness, clumsiness and pale skin.
Read: Fever | Common causes and when should you worry?
The flu cannot identify whether you are a man or woman, young or old, healthy or unhealthy. Almost every person is susceptible to cold-weather health hazards. However, there is a small set of people who are more vulnerable than others.
People who are at a higher risk of winter health problems include:
The safety challenges for the above group are higher than usual. People who fall under these categories should exercise added precautions.
Also, read: What is Coronavirus: symptoms | how it spreads | how to avoid it
These winter worries and health hazards can affect any person who does not rehearse proper caution. The following are some expert-advised tips to practice in order to prevent these illnesses:
Coronavirus has ensured that no individual is left unmasked. Nonetheless, wearing a mask does not only protect from COVID-19 but also these popular winter worries.
Seasonal illnesses like the common cold and flu are communicable diseases. They can easily transmit from one person to another. Protective gear like a face mask stops the transfer of the flu-carrying droplets.
Winters can be extra harsh on the skin. Dryness and itching of the skin is a very popular problem. One way to deal with this winter worry is to regularly moisturise your skin. You can use a light body lotion, body butter and homemade milk-based creams for this purpose.
Skin dryness can affect sensitive areas of your face as well, such as your lips. You can apply petroleum jelly for chapped lips. If the skin itching continues or develops into rashes, you should consult a dermatologist immediately.
People who confront endearing joint pain during winters should not entirely give up on exercising. You should choose to exercise indoors to keep your joints moving.
You can take online yoga or aerobic classes to keep up the habit of working out. You are advised to not put excessive pressure. If the pain increases, meet an orthopedist as urgently as possible.
Remember when your mother would dress you in childhood, she would always put on one extra layer of clothing. This trick may be old but very useful in preventing seasonal illnesses.
You should aim to stay as warm as possible, mainly while stepping outdoors. You should ensure to conceal most parts of your body. Protective winter wear includes warmers, caps, gloves, socks, scarves and more.
The Winter season gives us all the more reason to apply social distancing. The aim is to terminate the flow of viruses. By maintaining a healthy physical distance from each other, we can ensure that there is no transmission of diseases. You must make certain to practice this tip, especially while participating in a festive celebration.
Winter season calls for an increased need for sanitation and cleanliness. The different types of bacteria and viruses can latch on surfaces. They can further pass on from one person to another through these surfaces. It is necessary to properly clean and sanitise your surroundings if you wish to stay clear of health concerns.
One of the top tips to protect elderly from winter hazards is to feed them essential warm drinks. We tend to drink less water during cold weather. This habit can lead to dehydration and pose harm. Thereby, you should aim at drinking as many warm fluids as possible.
Warm water, tea (preferably green tea), vegetable or chicken soups and more should be consumed. You can also offer warm flavored milk to children and elders.
You can catch cold-weather illnesses more easily if you make rounds outdoors. This is why you should spend as much time possible in a moderately warm surrounding. You can utilise electrical room heaters to keep the environment cosy.
Winter health hazards can be effectively prevented by taking these safety measures. By carrying out these pointers, you will also keep yourself protected from the risk of coronavirus. These tips to prevent cold-weather winter hazards are practical and only require little attention.
For more information or personalised guidance, you can book an appointment with Internal Medicine expert at CK Birla Hospital.
Also, read: Tips to keep your child healthy and strong this winter

Nearly 3.8% of the Indian population is affected by some form of disability. Out of these, around 15-20% of physically disabled children live with cerebral palsy. Despite the high numbers, there is a lack of awareness about this condition among parents. In this article, – best pediatric Orthopaedic surgeon at the CK Birla Hospital discusses all you need to know about cerebral palsy meaning, its symptoms, treatment and more.
Here is everything you may need to learn about cerebral palsy.
Table of Contents
Cerebral Palsy is a group of conditions that affect the movement, posture or co-ordination in a person.
The word ‘cerebral’ means the brain while the word ‘palsy’ signifies problems in muscles. Collectively, cerebral palsy is understood as a set of chronic conditions associated with the brain that affect the functioning and growth of muscles in a child.
These lifelong conditions differ in each child. The part of the brain affected in every child is varying. Thus, a distinct movement disorder can be seen in different separate patients.
Medical experts have categorised mainly four types of cerebral palsy in children:
Spastic Cerebral palsy is among the most common types of cerebral palsy. It can affect a child before, during or after birth. Under this condition, the motor activity of a child is impacted. Spastic cerebral palsy is further divided into three types:
This classification is also known as dyskinetic cerebral palsy. Children who live with this condition who signs of both excessive stiffness and floppiness in their muscles. Athetoid is the second most common type of cerebral palsy.
Ataxic cerebral palsy majorly impacts a child’s coordination capabilities. As a result of ataxic cerebral palsy, children are unable to control their movements and form balance.
Mixed cerebral palsy is when a child displays symptoms of more than one type of cerebral palsy. They will have difficulties in balance, highly stiff muscles, floppiness among other issues.
Generally, cerebral palsy symptoms are detected after 2-3 years of the child’s birth. There is no fixed set of signs because every child is affected by this condition uniquely. However, there are some common cerebral palsy symptoms. These include:
Medical help is given to the child depending upon the type and symptoms of cerebral palsy.
There are multiple causes. Some children acquire this condition since birth. However, some children develop cerebral palsy after being born; usually immediately after birth or during the initial 1-2 years of life.
Some of the common reasons for what causes cerebral palsy in children are:
Every so often, the early cerebral palsy symptoms go unnoticed by parents. It is important to keep a track of the baby’s growth to detect any medical condition.
Self-diagnosis of cerebral palsy can be a starting point. Parents should carefully monitor their child’s movements and functionality of body parts.
It is possible that your child is a slow learner. You should not jump to a conclusion almost immediately. A consistent check on the child’s movements and growth should be kept.
Also, read: Finding the permanent solution for clubfoot
You should speak to your healthcare provider in case you detect a form of movement disorder in your child. Your doctor will examine your child’s health and do a thorough diagnosis.
There is a wide range of tests that are done to diagnose cerebral palsy. The type of tests performed depends upon the difficulty the child is facing.
Common tests and scans done to verify cerebral palsy in children are:
Brain scans: Imaging techniques like MRI, CT Scans and cranial ultrasounds. These are painless tests that may cause your child slight discomfort. They are used to develop detailed pictures of the brain.
Electroencephalogram (EEG): An EEG is done to check the electrical activity of your child’s brain. It is a safe test recommended for patients who suffer from seizures. A series of electrodes will be attached to the scalp of your child for this test.
Laboratory tests: Several types of tests like blood and urine tests will also be done as part of the diagnosis process.
Additional tests: A number of extra tests may be indicated to your child based on their specific medical difficulty. These include tests for:
Cerebral palsy in children is a lifelong condition that requires constant medical care. While there is no cure for these conditions, different treatment options are available that can help in managing the impact of symptoms.
Medicines – Specific medicines to treat muscle stiffness or floppiness can be given to children for the treatment of this condition. Mostly, medicines help in alleviating symptoms such as spasms, seizures and more. Muscle injections may also be offered by your doctor to help in tightening the nerves.
Physiotherapy – Physiotherapy is an important treatment option for cerebral palsy. Since it is a condition of the body movements, regular and specific physical exercises can help in improving motor function. Physiotherapy is also useful in the strengthening of muscles, improving flexibility and balance and enhancing movement.
Surgery – In some cases, surgical intervention may be required to treat cerebral palsy. There are some types of deformities that can be corrected with the use of surgery. Surgery can help in:
Occupational therapy – Occupational therapy is beneficial in supporting the child to perform everyday tasks. Under this treatment type, a therapist assists the patient in the functioning of routine activities.
Speech and Language therapy – Some children who affected by cerebral palsy also suffer communication problems. Speech and language therapy provides them useful ways of communicating in a better way.
There are numerous other types of therapies and remedial methods that depend upon the type of cerebral palsy. Behavioral therapy, treatment for drooling, aqua-therapy and more are constructive ways of supporting patients.
There is a common misbelief that cerebral palsy in children negatively impacts their life span. However, it is not true. A diagnosis of cerebral palsy does not affect the life expectancy of the child.
Nonetheless, children living with this condition will require continuous medical support throughout their life.
Cerebral palsy in children is a common movement disorder. It is significant to detect this condition at an early stage so that the right support can be offered to the patient. All new parents should pay attention to the bodily functions of their children. If they suspect any cerebral palsy symptoms, they should instantly seek clinical help.
For more information or personalised guidance, you can book an appointment with Paediatric orthopaedics and sports injury specialist at CK Birla Hospital.
You can also read about cerebral palsy in Hindi here.

Earlier, erectile dysfunction (ED) was only associated with feelings of guilt or shame. It was regarded as a sign of weak masculinity. We have, however, surpassed that stage and now ED is examined as a valid medical condition. Thanks to the constructive treatment modules, ED can be treated effectively similar to other health concerns. A penile implant is a successful and beneficial ED treatment method.
Dr Shalabh Agrawal, one of the best penile implant surgeons in Gurgaon, explores the subject of penile implant surgery in this article. Here is everything to know when considering a penile implant. Read on.
Table of Contents
A penile implant is a medical device. It is used to treat erectile dysfunction in men. This device allows an ED patient to experience an almost natural erection.
Doctors recommend the use of a new penile implant when other remedial options have failed. Generally, medications are prescribed as the first line of treatment.
Erectile dysfunction is treatable with the use of medicines or a penis pump. Nonetheless, sometimes a man cannot attain a successful erection to have sexual intercourse with these methods.
Doctors indicate penile implant when the above-given methods fail. If a patient is not satisfied with the results of these treatments, he can also choose to opt for surgery.
Besides ED, a penile implant is also used in the treatment of painful erections. You can have an implant surgery if:
A penile implant is also known as a penile prosthesis. There are majorly two different penile implants used by surgeons.
Penile implant surgery is indicated to a patient as a last resource. The type of penile implant depends upon the patient’s choice and his medical conditions in the past. Your doctor will assist you in making the right selection.
An inflatable prosthesis is built of two cylinders, a reservoir and a pump. All three parts of this implant are placed in different parts of the body.
The cylinders are surgically placed inside the penis. While the reservior of fluid is inserted under the lower abdomen area. The cylinders are attached to the reservoir through a tube. The pump, however, is implanted under the skin of the scrotal sac between the testicles.
To have an erection, a man only has to press the pump of the implant. As the pump is pressed, the reservoir fluid is transferred to the cylinders inside the penis leading to an erection.
A semirigid rod always maintains its stiffness and size. Once implanted, the rigidity of the penis remains intact. However, this implant can easily help change the position of the penis. It can be bent comfortably due to its half-stiffness.
When a man needs to engage in sexual activity, he can simply bend the penis forward. When he needs to conceal himself, he is required to keep the penis towards his own body.
Penile implant surgery is a relatively safe procedure. Nonetheless, as with any surgery, there are some risks associated with it.
Infection: The rate of infection in the case of a penile prosthesis is low. However, the chances of infection increase if the patient is diabetic or suffers from a spinal cord injury. Penile implant problems such as an infection are manageable. Infection occurs during the first few weeks post-surgery. Common signs of an infection from the penile implant are fever, a build-up of pus and swelling in the scrotum area.
Penile implant problems: There is a likelihood of implant problems if the prosthesis is broken or does not function properly. If this issue arises, your doctor would remove the broken device and replace it with a new penile implant.
Implant erosion: A penile implant can experience erosion from the inside. The device can stick to the penis and cause skin problems. Internal erosion of the implant is an extremely rare problem.
Other risks of penile implant surgery include:
A penile prosthesis surgery is not a complicated procedure. Before the surgery, you should consider the following to take place:
This procedure can be done at CK Birla Hospital where you can find the best penile implant surgeons in Gurgaon.
Your surgeon will offer anesthesia to help reduce pain from the procedure. The surgical site will be prepared by clipping off extra hair to decrease the risk of infection.
The surgeon will make an incision (cut) to implant the device. It could be at the base of the penis, below the head of the penis or in the lower abdomen. Based on the preferred type of penile implant, your surgeon would do the positioning.
Afterward, your surgeon will carefully sew back the incision as the procedure completes.
After the procedure is performed, you can expect the following:
Also, read: Premature ejaculation-causes and symptoms
Penile implant surgery has good success rates. If performed by clinical experts in a hygienic and well-maintained operative theatre, the surgery is effective in 90% of cases.
Most men are able to retain their sexual function and perform better sexually, after an implant.
The type of penile implant is important in knowing if the device will be noticeable. In most cases, the patients only experience small scars from the surgery. Besides scarring, an implant is hardly distinguished.
A penile prosthesis can function effectively for up to 10-15 years. The role of the surgeon is very important in making sure that the implant is fixed properly. The risks associated with this procedure can be considered the disadvantages of penile implants. The surgeon should be able to minimise the probability of these risks.
Penile implant surgery is a credible solution to a rather embarrassing condition like erectile dysfunction. A single procedure can last for over a decade. It is also extremely safe if operated with clinical care.
For more information or personalised guidance, you can book an appointment with Dr Shalabh Agrawal, Consultant – Urology and Andrology at CK Birla Hospital.

A bunion (or hallux valgus) is a deformity on the metatarsophalangeal (MTP) joint. Bunions can be unsightly and even painful in severe cases. It can develop in people of all ages. Dr Praveen Tittal leading orthopaedic surgeon and one of the best foot specialists in Gurgaon sheds more light on the causes of bunions, their treatment and how can you prevent this painful deformity.
The metatarsophalangeal joint (also known as the MTP joint) connects the toes to the main part of your foot. In some cases, the bones, ligaments and tendons in this joint can move out of place causing the big toe to get pulled towards the smaller toes. This misalignment disrupts the equal distribution of your weight on the joint resulting in instability and deformity in the joint.
The exact causes of bunions are still unclear. However genetic factors, underlying conditions and trauma or stress to the foot are known to contribute towards bunion formation. In the following section, these factors are explained in further detail.
Bunions might run in families. However, having a family history of bunion does not necessarily mean you will develop them as well. However, there is a higher risk of bunion formation due to inherited poor foot mechanics or shape. In such cases, extra care needs to be taken to prevent bunions from forming.
In extremely rare cases, babies may be born with bunions. This condition is also referred to as congenital hallux valgus. The causes of this are thought to be genetic. In mild presentations, it can be treated non-surgically with treatments such as corrective footwear. In more severe presentations, surgical treatment options are recommended. It is sometimes detected during prenatal ultrasound scans.
Conditions that can cause inflammation and pain the joints such as rheumatoid arthritis can also contribute to bunion formation. Diabetic people are also more prone to developing this deformity.
Sudden trauma to the foot or constant stress on the foot for a prolonged period of time (years) can also result in misalignment of the MTP joint. Experts also believe that prolonged use of ill-fitting or high heeled shoes can also put you at a greater risk of developing bunions, especially if you are already prone to it.
Read: 12 everyday tips for foot care in diabetes
The first and foremost step to treat bunions is to relieve the pressure on the MTP joint.
The most basic way to relive the pressure is to use the right kind of shoes. There are three factors to consider while selecting shoes for daily use. The form, fit and function.
The form is the visual aspect of the shoe and is more or less inconsequential to foot health. Fit and function on the other hand are vital to ensuring healthy feet.
Fit indicates how the shoe accommodates the shape of your foot. While ensuring that the shoe fits your foot lengthwise is not tough, finding shoes that are not too loose or tight breathwise can be challenging. This is also due to the fact that our feet are prone to changing their shape as we age.
Function refers to the shoe’s purpose. In many cases, shoes are designed especially for a particular activity. For example, sandals may not be the right shoes for a basketball game.
Also, read: Learn more about how to select the right pair of shoes
Another aspect of choosing the right shoe is ensuring the right amount of support and cushioning to the feet. Choose a wide, flexible sole with a sturdy heel counter. You can use stretchers to reshape narrow shoes if they feel tighter with time. For patients requiring extra care like diabetic patients, custom-made shoes can be a good option.
If you are experiencing mild discomfort or pain due to your bunions, you can use gell filled pads and over-the-counter painkillers. Patients also experience some relief by warm soaks, icepacks and massages.
In extreme cases, doctors can also recommend surgical correction of the deformity. For milder cases, a procedure called bunionectomy is performed. It involves shaving of the prominent bump along with realigning the soft tissues around the big toe. For moderate to severe deformities, an osteotomy which involves cutting the bone, realigning and fixing it back with screws or plate is performed. The outcome of successful surgery is improved function, a well-positioned big toe and pain relief.
If treated at a lesser stage, bunions can be corrected with minimally invasive surgery. This procedure is associated with lesser pain and quicker recovery.
Taking the right care of your foot after bunion surgery is an important deciding factor of the outcome of the procedure. After the procedure, the doctor holds the toe in place using a firm dressing. Keeping the toe in place is essential for the realignment of the toe. You would be advised to keep your foot dry and clean. Remember not to remove or change your dressing without consulting your doctor.
After the surgery, patients are advised to keep their feet in an elevated position for a few days. Keep pillows or cushions under your foot to keep it elevated. You would also have to wear special shoes that are designed to redirect the pressure of your body to the heel instead of your toes.
In some cases, you will be allowed to walk right after surgery. However, you would be required to wear special surgical shoes to protect the correction.
While bunions rarely cause complications that inhibit our daily lives, they can be irritating and painful. Prevention is better than cure. Remember to use the right kind of shoes, maintain healthy body weight and perform specialised exercises focusing on your toes.

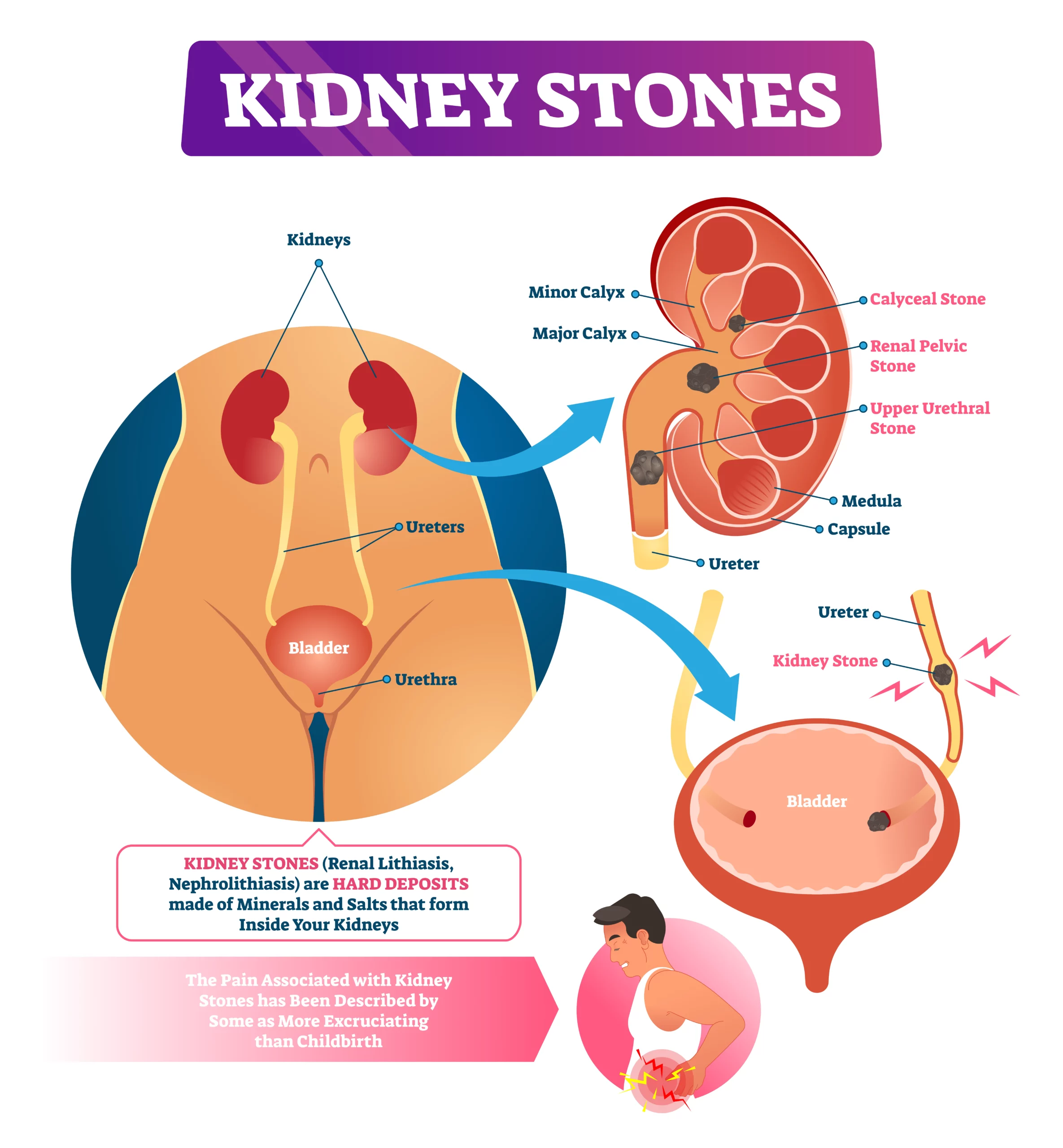
Children are funny creatures with strange interests. They like playing in mud or eating dirt. We are all guilty of falling for these games at some point in time. As little kids, we were told that our bellies will fill with stones if we eat impurities. Apparently, this make-believe story has an aspect of real life. Kidney stones are tiny rock-like objects that get collected in the kidneys.
The development of kidney stones is a very common condition. Nearly 1 out of every 10 individuals are affected by signs of kidney stones. This article explores kidney stones symptoms, signs and prevention in detail.
Dr. Mohit Khirbat, a leading nephrologist in Gurgaon, provides his insights on how to prevent kidney stones naturally.
Kidney stones are crystal-like substances that form inside the kidneys. They develop in varying sizes and shapes and range from minuscule like a grain of salt to large stones like a chickpea. They are made up of small substances that are usually found in urine.
Kidney stone prevention can be done without medical intervention also. However, it is necessary to first acknowledge its signs and symptoms.
Some stones are microscopic in mass. Due to this aspect, the symptoms usually go unnoticed. However, even these mini objects can expand later. They may also move within the organ causing pain and discomfort. Therefore, it is important to learn about the symptoms of kidney stones.
Here is a list of the most common sign and symptoms of kidney stones:
Apart from the above-given symptoms, the following are also signs of kidney stones-
It is advised that you seek immediate medical help, if:
Kidney stone pain is located at the lower abdomen or groin, along one side of your body and below the ribs.
There is no exact cause of kidney stones. It is known that certain substances in your urine lead to the production of kidney stones. The various types of kidney stones determine their individual causes.
While kidney stones can develop in anyone, some people are at a greater risk than others.
Risk factors of kidney stones include:
Read: Kidney transplant during the COVID pandemic
The strategy that ‘prevention is better than cure’ applies to kidney stones as well. In fact, kidney stone prevention is rather a matter of lifestyle changes. According to nephrology experts, here are some ways you can avoid kidney stones.
As mentioned earlier, kidney stones are not always diagnosed unless they cause health issues. Sometimes, patients live with small-scale stones for years without knowing. Therefore, the diagnosis is often delayed. The patient is informed about the condition after it has progressed. In such cases, both treatment and prevention can be offered to get the desired clinical results.
Prevention of kidney stones with the use of medicines depends on various factors. There are distinct types of kidney stones. For instance, calcium stones, uric acid stones, cystine stones, struvite stones and more. Doctors prescribe medications for condition-specific issues.
Kidney stones are not a modern disease. As preventive healthcare is gaining popularity, protection has become the key aspect. However, we cannot focus on preventing a condition unless we recognise its existence first. Thereby, a basic understanding of kidney stone symptoms is a must.
Afterwards, a focus on prevention is chief to avoiding kidney stones. A healthy way of living that includes sufficient hydration, a nutritious diet and exercise is the ultimate solution. For information or personalized guidance, you can book an appointment with Dr. Mohit Khirbat at CK Birla Hospital.

Even the thought of going through surgery is overwhelming. Imagine experiencing the complications from the said surgery. Though there has been revolutionary growth in healthcare, this field is not exempt from failures. A common example of such blunders is the prevalence of knee replacement surgery failure.
Knee replacement surgery, also known as knee arthroscopy, is a conventional and effective surgical treatment for conditions like knee arthritis. The average span of the impact of this treatment is about 15-20 years. However, some risk factors of knee replacement surgery can lead to its failure.
In this article, Dr Ashwani, one of the best knee replacement surgeon in Gurgaon, provides his insights on why a knee arthroscopy fails?
Table of Contents
During knee arthroscopy, surgeons cut open the affected knee for repair. They remove the damaged surfaces from the joint and cap the joint surface with metal and plastic implants.
There are numerous factors why do knee replacements fail. In some cases, more than one factor is responsible for the impairment. Here is a list of the top causes behind knee replacement surgery failure:
There is a variety of reasons why a knee arthroscopy damages. Some of these causes are beyond the patient’s control. However, most of these risk factors of knee replacement surgery failure can be avoided by practicing vigilance.
Here are a few ways knee replacement surgery recovery tips that can be maintained to avoid failure:
In most cases, knee replacement surgery failure occurs after 5-8 years of the procedure. After this gap, it is not very likely for patients to ignore the signs at the surgical area. The symptoms of knee replacement failure include:
Read: The risk of delaying Knee Replacement Surgery
Knee replacement surgery failure can be further treated successfully. Needless to say, the patient is required to take exceptional care if a revision treatment is recommended.
If and when a knee replacement surgery failure happens, revision surgery is done. It is similar to the original knee arthroscopy but aims at eliminating the factor that has lead to the failure.
In a revision surgical procedure, surgeons remove the pre-installed implants and replace them.
A revision knee replacement surgery failure is typically divided into three phases:
The recovery process of revised knee arthroscopy is similar to knee replacement surgery. Primarily, the patient would be kept under observation to keep a check on further improvements or complications.
Recovery tips for a corrective knee arthroscopy consist of:
Note: The length of the recovery period varies among patients.
Read: Quality of life after Total Knee Replacement Surgery
Knee replacement surgery failure is an ordinary medical complication. In the recent past, there has also been a rise in the number of revision surgeries.
For information or personalised guidance on knee arthroscopy, you can book an appointment with Dr Ashwani, best knee replacement surgeon in Gurgaon.
Read: Partial vs total knee replacement surgery: Which fits better?

Earlier women who delivered via a cesarean section had no other option other than opting for a cesarean section for all subsequent pregnancies. Today, VBAC or vaginal birth after caesarean offers an alternate birthing process for women. In this article, Dr Anjali Kumar, top obstetrician and gynaecologist in Delhi NCR talks about 5 things everyone thinking of VBAC should know.
Table of Contents
Before opting for VBAC, you need to assess if it is the right option for you. Some risks can make it an unviable birthing option. There are several factors that decide if you are an ideal candidate for VBAC. These include:
The three types of uterine incisions used for C-sections are low transverse, low vertical and classical uterine incisions. VBAC is usually done only on women with low transverse or low vertical uterine incisions. A high vertical incision or classical incision is associated with a higher risk of uterine rupture.
Uterine rupture is a rare but severe complication that can occur in pregnancy. It causes the uterus to tear which can allow the fetus to slip into the abdominal cavity. Women with uterine scars due to previous caesarean sections are at a higher risk of developing this complication. If you have a history of uterine rupture, you would not be considered an ideal candidate for VBAC.
If you have undergone any surgical procedures on your uterus in the past such as fibroid removal, you would not be considered for VBAC. Previous surgeries can cause uterine scarring which is not ideal for VBAC.
VBAC is not recommended for women who have had more than two C-sections previously.
VBAC is not recommended for women who have undergone a C-section delivery less than 18 months prior.
If you have any other underlying condition such as placental problems or multiple births, which can complicate your pregnancy or labour, you would not be recommended a VBAC.
Other factors such as being overweight, breech presentation of the baby, size of the baby etc can also result in VBAC being ruled out. Discuss your suitability for VBAC at length with your obstetrician early on in your pregnancy so you can start preparing for your labour.
Read: Caesarean section delivery – What to expect
While you may be keen to explore the option of vaginal birth after caesarean (VBAC), the fact is that not all hospitals or doctors offer this birthing option. While complications arising from VBAC are rare, hospitals and doctors need to be prepared to perform an emergy C-section during TOLAC (Trial of labour after cesarean). Constant fetal and maternal monitoring is also essential during this process. Hence, if the hospital or doctor is not experienced in handling difficult labour, they may not offer VBAC as a birthing option. Deciding to switch your hospital and doctor later in the pregnancy can be tough. Hence, choose your hospital and doctor after exploring these options carefully, early on in your pregnancy.
In the past few years, there has been a sharp increase in the popularity of VBAC. Many expectant mothers wish to explore this birthing option due to the number of benefits associated with it. Lower recovery time, lower risk of infection from the surgery, shorter hospital stay and lesser pain are some of the advantages of VBAC for the mother. Even for the baby, passing through the birth canal helps squeeze the fluid from his/her lungs as well as transfers good bacteria, providing him/her valuable immunity after birth.
A lesser-known fact about caesarean section is that it is not ideal for women wishing to give birth more than 3 times. As repeated cesareans can cause several complications and uterine scarring. Each consecutive c-section poses a greater risk than the previous one. In such a scenario, talk to your doctor about your birthing options.
Like any other medical procedure, VBAC also has several risks associated with it. This is one of the major reasons why it is not ideal for everyone, nor is it offered by all medical institutions and doctors. Complications arising from VBAC are rare, also because the candidate for VBAC is screened thoroughly to minimise their risk factor.
During a VBAC, there is a small chance that the previous uterine scar breaks open. This occurs in less than 1% of all VBAC deliveries. In such a case, an emergency hysterectomy might have to be performed. There is also a chance that the VBAC attempts have to be abandoned midway due to maternal or fetal health. Emergency C-sections is performed in such a scenario.
If you have assessed your suitability for VBAC, start preparing for it early on. Speak to your doctor at length about steps you can take to have a healthier pregnancy and reduce the risk of developing pregnancy complications. Ensure that your hospital is equipped to handle complications during childbirth and also has a good NICU. Speaking to other women who have also undergone VBAC can help you manage your expectations and be better prepared.
For more information about prenatal care and birthing options, you can consult Dr Anjali Kumar at the CK Birla Hospital.